Book
Do robots have a bright future in public health?
When her mother was in a rehab facility, Daniela Rus noticed that transporting patients was a major bottleneck; they were constantly waiting for a person to come with a wheelchair. She quickly formed an idea: “I believe that with today’s technology, we can build autonomous wheelchairs and gurneys capable of transporting people efficiently.” Her team even built a prototype and tried it out at a rehabilitation site. Rus hopes such an innovation could improve efficiency in hospitals.
Rus is the head of the MIT Computer Science Lab and a recently elected member of the National Academy of Sciences. Her new book, The Heart and the Chip: Our Bright Future With Robots, written with science writer Gregory Mone, makes a case for robots as a source for opportunity and growth in human life.
Harvard Public Health spoke with Rus about some of the critical questions around robots and public health, including the ways in which they are impacting medical procedures, health care, and two other areas influential to human health—employment and the environment.
This interview has been edited for length and clarity.
HPH: What’s a good example of how robots are already impacting the health world?
Rus: There is a project in Germany called Brainlab. I visited this group last year, and I was completely blown away. These scientists are using robots to do spinal surgeries which are very, very delicate. The surgery involves the placement of screws in the spine, and the screws have to be placed very precisely because otherwise there is the risk of nerve damage. There is a very interesting symbiosis between doctor and machine in this application.
The process works like this: A doctor images the spine; a planning algorithm helps determine where the screws will be placed; and a surgeon then makes corrections to the plan. Then a robot takes over to implant the screws, under the supervision of the doctor. The robot can move with greater precision than the human. The robot augments the human’s precision, and the human augments the reasoning of the machine.
Sign up for Harvard Public Health
Delivered to your inbox weekly.
Of course, robots have been used for surgery and for training for a long time. The da Vinci system was introduced more than 20 years ago, and this type of robot is in so many hospitals. The[se] surgical robots are ensuring that the incisions are minimal, which also prevents the risk for infection and . . . makes healing faster. The other benefit of the da Vinci robot is to enable experts to perform surgeries remotely, which has been really important for bringing equity and inclusion to medicine.
But despite these advances, I would not suggest that autonomous robots should independently decide whether to cut or not cut in a surgical setting. I wouldn’t yield that level of control to machines.
HPH: You had a front row seat during the pandemic for some wild—and wildly quick—innovations with robots. Do you think we’ll be turning over things like pandemic response to robots any time soon?
Rus: During the pandemic I worked with Ava Robotics to develop UV-disinfecting robots. The robot traveled through the space to be disinfected—a warehouse or a COVID testing facility—using our coverage algorithm. Its UV light reached all the visible surfaces and killed the viruses and bacteria on those surfaces. Especially at the beginning of the pandemic when we didn’t know much about the virus—how it was transmitted, how long it survived on surfaces—having this autonomous disinfection platform was very appealing.
We deployed these robots at the Boston Food Bank to support both the staff working there and the many first responders who relied on the food bank for their meals. We also had these robots deployed in the MIT Covid testing facility.
HPH: You were also involved in an innovative open-source project that deployed robotic help for ventilation in hospitals during the pandemic.
Rus: Within about a month—during March and April, when the pandemic started—we built a robotic ventilator which we called the MIT Emergency Ventilator. So if you remember, at the time, people were dying because there weren’t enough ventilators, and fabricating more ventilators was just not possible with the current processes that companies had available. What we had, however, were ambu-bags, these plastic bags that are very inexpensive and are placed in every hospital room and every ambulance. These bags are meant for manual ventilation for a little bit of time while you transport a patient.
People with COVID-19 who needed ventilation required it not just for a few minutes, but for days on end. So, we built a robotic ventilator. Think of two robotic paws capable of squeezing the ambu-bag at the correct rate for each individual patient. This low-cost solution was deployed in a hospital in New York. We also published the blueprints, designs, and code for the system. Throughout the process, we worked closely with doctors to ensure that the ventilator had the right sensors, provided the necessary feedback, and featured an interface that doctors could easily use.
Developing the robotic emergency ventilator was possible because we understood the problem; it was a moment of crisis, and our students at MIT stepped up and spent a few weeks creating this custom solution for a humanitarian need. By open-sourcing the designs, we enabled many teams around the world to adopt and implement the solution.
HPH: Public health is not the same as medicine; you could think of unemployment or the falling costs of certain services as being a public health question. Are there things coming in the next few years that are going to have big social impacts?
Rus: Jobs are constantly evolving. And I believe that it’s much easier for people to think about what will go away than to think about what will come. My belief is that certain aspects of jobs will be taken over by machines, which is beneficial because those tasks are often not well-suited for people. This shift will allow people to focus on the tasks more suitable for people and pursue a wider variety of other types of jobs.
A very useful example to keep in mind is what happened with the digital revolution . . . around the year 2000, when the dot com boom was in full force, nobody was talking about smartphones or about cloud computing or social media. These three technologies were all introduced in the year 2007, not that far into the future. And they opened the door to so many jobs, and not just geeky jobs: content creators, designers, such a wide range of professions benefited from the advancement of these jobs. And new jobs that didn’t exist were created. Similarly, in public health, advancements in technology and data analytics have created roles in epidemiology, health informatics, and telemedicine that didn’t exist before, enabling more effective disease tracking, patient care, and health policy planning.
Book cover: WW Norton
More in Tech & Innovation
A farewell to HPH readers
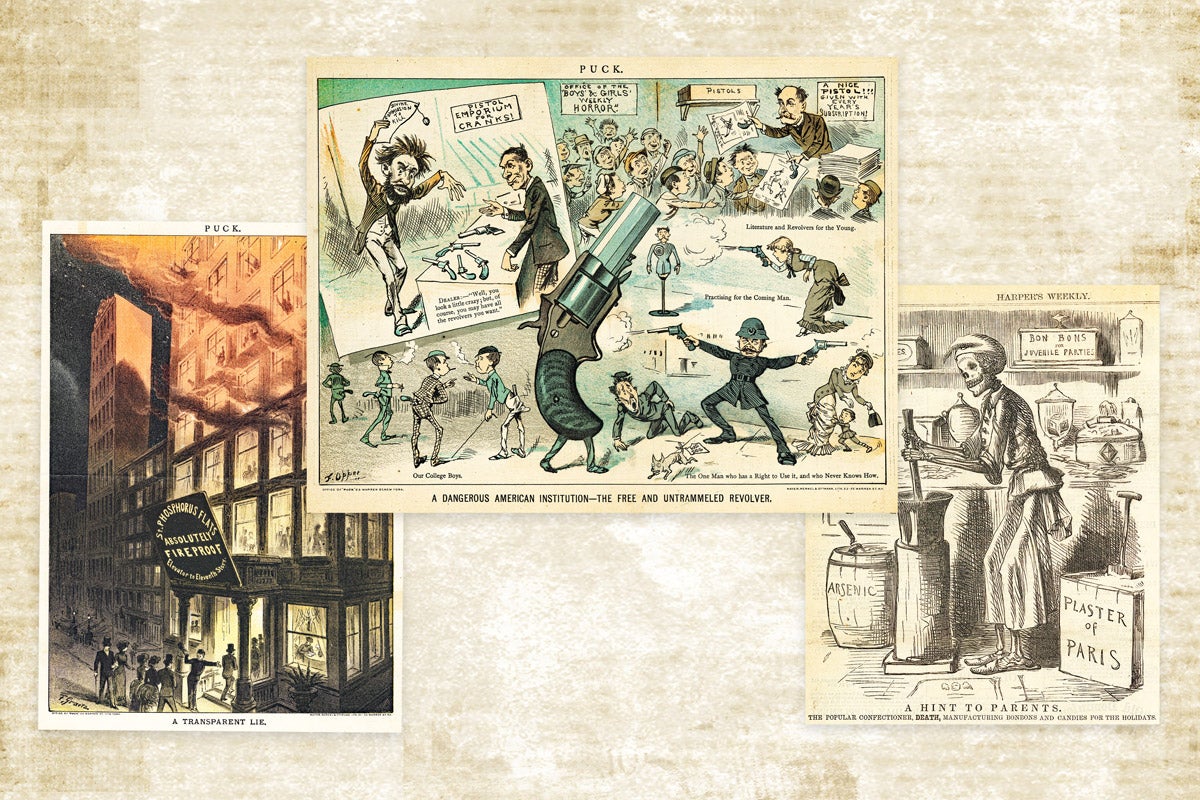
Editorial cartoonists were early U.S. public health advocates
