
Feature
Weaving data into the fabric of public health
In 2017, Maryland’s Department of Health found funding for a program to send caseworkers to the homes of asthmatic children to help get their disease under control, but they had a problem: finding the kids.
Targeting infectious diseases like influenza or lead exposure would have been easier: State laws required reporting those illnesses to public health officials. But asthma is a chronic disease that health care providers weren’t required to report. How could caseworkers find the children they wanted to help?
Clifford S. Mitchell, director of the office that led the program, first looked to Medicaid claims data since the asthma program was intended for low-income kids. But that data was only reported every six months, and then it had to go to a vendor to be analyzed—which meant as much as a year may have passed between a child’s visit to the hospital and the first outreach by a caseworker. By then, contact information for the families often no longer worked. If their children hadn’t just had an asthmatic crisis, parents often saw no need for a caseworker to visit their home. “We [had] a conundrum, because we have this service,” Mitchell remembers, “but we can’t really efficiently get to the people who are most likely to receive the service favorably and ask for it.”
He found a solution in a system that wasn’t created for public health at all: a health information exchange, initially set up in the mid-2000s to organize and share patients’ electronic health records between their health care providers. Maryland’s health information exchange, known as CRISP, received hospitalization reports every night. It could identify Mitchell’s target patients in real time.
Sign up for Harvard Public Health
Delivered to your inbox weekly.
It took some effort to work out technical and privacy issues to integrate CRISP’s data into systems used by the state health department and county-level case workers, and the program slowed dramatically during the COVID-19 pandemic. But on September 8, 2022, information about children eligible for the asthma program began moving automatically from the CRISP database to the county caseworkers who could reach out to families. Caseworkers were suddenly enrolling about 25 percent of children the system flagged for the program—a success rate roughly ten times higher than when they were working with Medicaid claims records.
“I am one lucky guy,” Mitchell says. He has the real-time ability to track an illness and deploy an intervention that most public health workers only dream about. He is also working in a state that has taken steps to make it especially easy to adapt a health information exchange (HIE) built primarily for health care providers so that it serves a public health function.
Maryland is one of 43 states that rely on HIEs for at least one public health function, according to a 2022 study published by the Civitas Networks for Health, a national collaborative of organizations working on HIEs. Providers, payers, and public health officials are gradually recognizing the whole health system, public and private, can benefit if they share tools with one another.
For many years, there have been two entirely separate conversations about data modernization in health care—one among public health agencies used to working with disease registries based on reporting requirements imposed on health care providers, and a parallel conversation among doctors, hospitals, and health plans working to streamline patient care. There’s a growing recognition, especially after the pandemic, that both communities are wrestling with the same question, and there are many ways they could work together—to make practitioners’ lives easier and to improve the nation’s health.
Using CRISP for poor kids with asthma would have seemed far-fetched when it began taking shape in about a decade earlier, because it was originally created to shuffle the medical paperwork of seniors. The data-sharing initiative spawned from the frustrations of John C. Erickson, the founder and then-chairman of a chain of elder care facilities called Erickson Senior Living. He didn’t like that when nursing home residents went to the hospital, the hospital’s doctors “would know nothing about them,” recalls David Horrocks, then Erickson’s chief information officer, “and then they come back, and our docs would know nothing about what happened in the hospital.”
Most information-driven industries were then rapidly adopting technology, like email, that’s now commonplace; medicine was still in the Stone Age, with practitioners relying on paper records and fax machines. Erickson thought there had to be a better way. In 2006, he enlisted Maryland’s three largest hospital systems to launch pilot programs to digitally share seniors’ medical records, and he put up $5 million of his own money to get it off the ground. Horrocks, as Erickson’s tech chief, was tasked with building the platform. Over several years, CRISP was developed.
It coalesced as lawmakers were trying to drag the health care industry toward the latest innovations of the information age. A major shot in the arm came as part of the economic stimulus package signed by President Barack Obama in 2009, which included the Health Information Technology for Economic and Clinical Health Act (HI TECH for short). The legislation codified a position in the Department of Health and Human Services (HHS) to coordinate health technology efforts and appropriated $35 billion over ten years to encourage the adoption of electronic health records—and HIEs to share records between providers.
None of these efforts paid much attention to public health; policymakers were focused on making providers more efficient, bringing down the cost of care, and improving patient outcomes. The federal government did not specify what form the HIEs should take, so they evolved in many different ways. Some were for-profit companies, some were independent nonprofits, and some sat inside state or county agencies. Some covered entire states while others were organized at a regional level or only included a subset of providers. Some were more focused on networking hospitals; others were more focused on serving health insurance companies. Collaborations between different stakeholders were often uncomfortable, because they required competing providers to share data with one another, as well as greater transparency between providers and insurers. In some states, privacy laws had to be modified to facilitate information exchange. And in some parts of the country, these challenges were so insurmountable that they are still not served by an HIE.
Maryland was fertile ground for building an especially robust HIE. The state already had a unique payment model in which an independent commission appointed by the governor sets payment rates for hospitals. The administration of then-Governor Martin O’Malley helped get all the state’s hospitals on board with CRISP, in 2009, and provided funding to keep it going. Maryland made a major change to its payment system in 2014 that allowed hospitals to keep more revenue by keeping patients healthier and using fewer services. That in turn meant hospitals needed better data tools to track their patients, and CRISP was ready to fill this need.
CRISP gave every hospital and provider a tracking dashboard and even real-time alerts when a patient went to the ER or was admitted to the hospital. Over time, these tools expanded to gather data from medical and mental health case managers. “If there’s somebody who can get help so they’re not admitted every week to the hospital, going from ER to ER, finding out who that person is and helping them becomes a really good thing for the health care system,” says Joshua Sharfstein, a medical doctor and professor at Johns Hopkins Bloomberg School of Public Health, who was Maryland’s health secretary as this system was being created in 2014.
For public health workers, CRISP can map hospitalizations for conditions like asthma to identify hot spots with much more precision than previous tools—and with actionable information. CRISP also runs the prescription drug monitoring platform for the state Department of Health. Its role is so central to Maryland’s health system that it is recognized as what’s known as a Health Data Utility, bedrock infrastructure that provides health information to many players in the state’s health care and public health ecosystem.
HIEs like CRISP, if widely deployed, could radically improve the practice of public health in the US, says Craig Behm, CRISP’s CEO. For instance, heat maps are a mainstay of public health. But they identify very broad geographic hotspots, which Behm says often doesn’t tell public health workers very much they don’t already know. “The [bigger] problem is, ‘What are the compounding factors and health related social needs and different outcomes? And where do people get care? Those details are available!… We need to go deeper now and we can.”
That level of information is available with CRISP. But “public health has been so undervalued and underfunded for so long,” Behm says, “Public health [officials are] having trouble even understanding what modern infrastructure could do for them.”
The COVID pandemic made painfully clear the high cost of underinvestment in public health data infrastructure. Federal budget allocations also show what a low priority such resources have been for policymakers. In 2009, for example, Congress appropriated $35 billion to advance data tools for providers and insurers. But it didn’t earmark money for CDC data modernization until 2019 and has only appropriated a total of $1.35 billion for the effort over the last four years.
The COVID pandemic made clear just how useful CRISP could be for public health, Behm says. Very early in the pandemic, CRISP was processing massive amounts of data every night, tracking case reports, hospitalizations, and deaths. Lab workers were sending incomplete demographic data to local Departments of Health, but CRISP could match the health department registries with its own data set, tracking in real time essential data like the race and ethnicity of infected Marylanders. When public health workers needed phone numbers to do contact tracing, Behm recalls, “I was like, ‘Well, great! I have all the phone numbers in the world!”
In the scramble to respond to COVID, other states’ public health workers also turned to HIEs as partners—often in ways they never had before. HIEs were glad to help, but those relationships became strained as the crisis passed, says Jolie Ritzo, Civitas’s vice president for strategy. “The challenges feel bigger than they were,” Ritzo says.
HHS is now steering the next evolution in the health information ecosystem, laying out standards and certifications for national information exchanges that will allow records to follow a patient from one HIE to another. At the same time, the CDC is leading its own Data Modernization Initiative and has signed contracts for hundreds of millions of dollars with Palantir to build a data system of its own.
A major open question is how these two efforts will interact. Many HIE leaders hope that existing data exchange infrastructure can link the information networks many providers already use regularly with upgraded data systems for public health officials. Erica Galvez, CEO of Manifest Medex, California’s largest HIE, and a former official in the health technology office at HHS, says she believes many public health departments will look to existing HIEs as an “on ramp” to the nationwide network.
Claudia Williams, who was Manifest Medex’s founding director, says HIEs have already done a lot of work to manage the complicated relationships between stakeholders at the local, regional, and state levels. It would be in everybody’s interest, she thinks, for the CDC to try to engage with the HIE infrastructure that exists rather than trying to develop an entirely separate information system.
“The better place to start is to strengthen and incentivize what goes on at the state level,” says Williams, who also served as senior advisor of health innovation and technology in the Obama administration and is now the chief social impact officer of UC Berkeley’s School of Public Health.
But fewer than half the states have HIEs ready to take on full public health functions at this point, says Horrocks, who left CRISP in 2022 to build a state-wide HIE in New York. (Horrocks also coauthored the nationwide study of HIEs published by Civitas in 2022.) Still, he believes they’re the best structure for public health to rely on in the long term.
“HIEs do something that’s very unique: We hold fully identified data in trust, and that lets us put datasets together,” Horrocks said. “I don’t know who else can do that. We’re not going to trust the … the state government, and you’re certainly not going to trust CDC to hold everybody’s fully identified data. And, I don’t think you’re going to trust Google to do it, either, or Palantir. I think that’s a role that these HIEs can uniquely fill.”
Image: berCheck / Adobe Stock

More in Tech & Innovation
A farewell to HPH readers
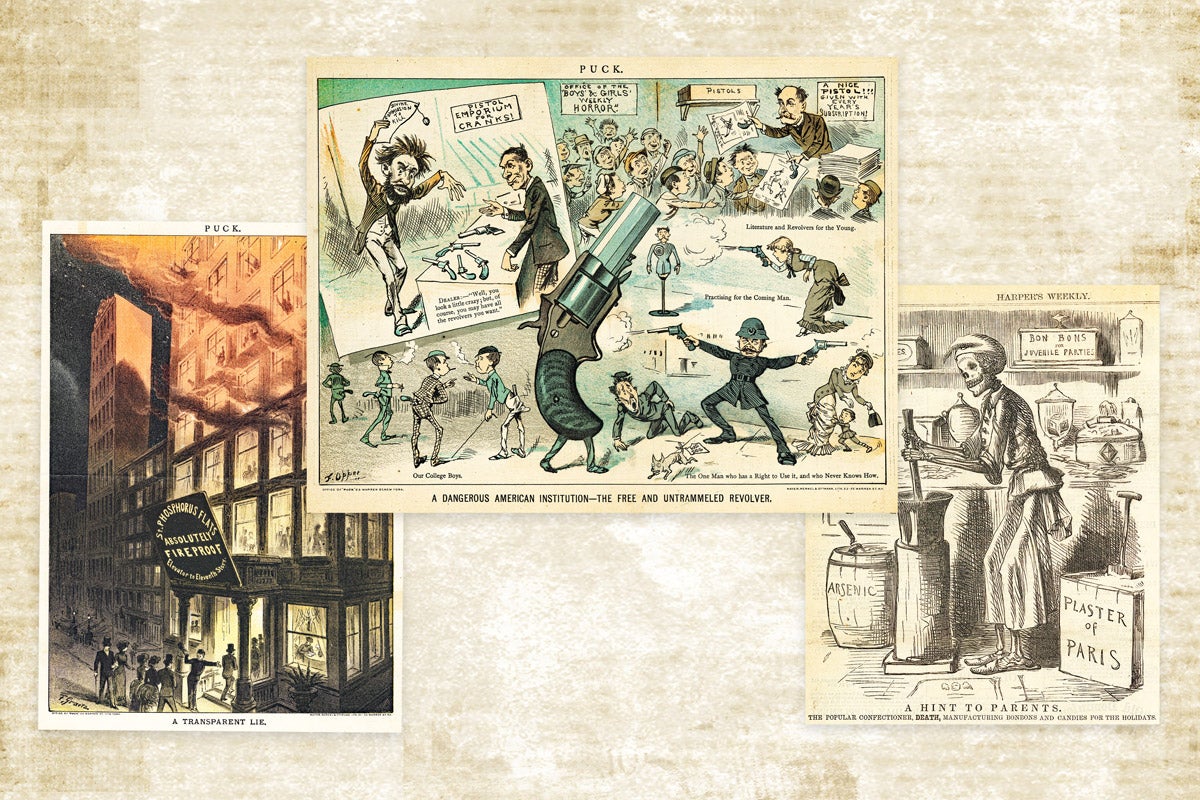
Editorial cartoonists were early U.S. public health advocates
